Breaking News




Popular News




Enter your email address below and subscribe to our newsletter

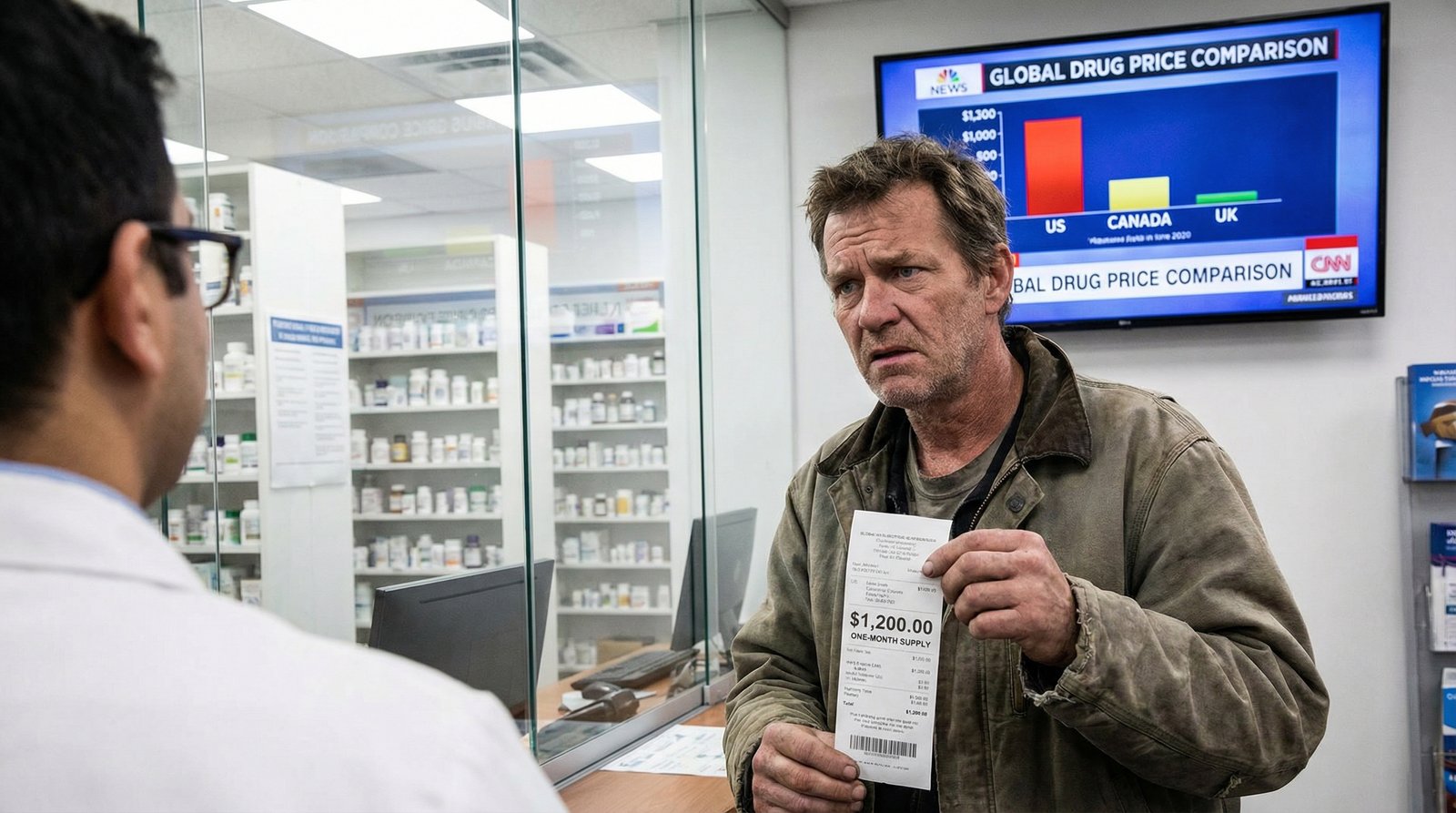
Prescription drug prices in the United States are the highest in the developed world — not slightly higher, but 3 to 10 times more expensive than the same drugs sold in Canada, Germany, or Japan. Americans spent $805.9 billion on prescription drugs in 2024, and 21% of U.S. adults admit they didn’t fill a prescription last year because they couldn’t afford it. The system isn’t broken by accident. It was built this way — and the generations that built it aren’t the ones paying the price.
Key Takeaways
- Americans pay $1,491 per capita annually on prescription drugs — 67% more than Germany, 50% more than Canada
- 21% of U.S. adults skipped filling a prescription last year due to cost
- Insulin costs over $300 per vial in the US — and $35 in Canada for the same product
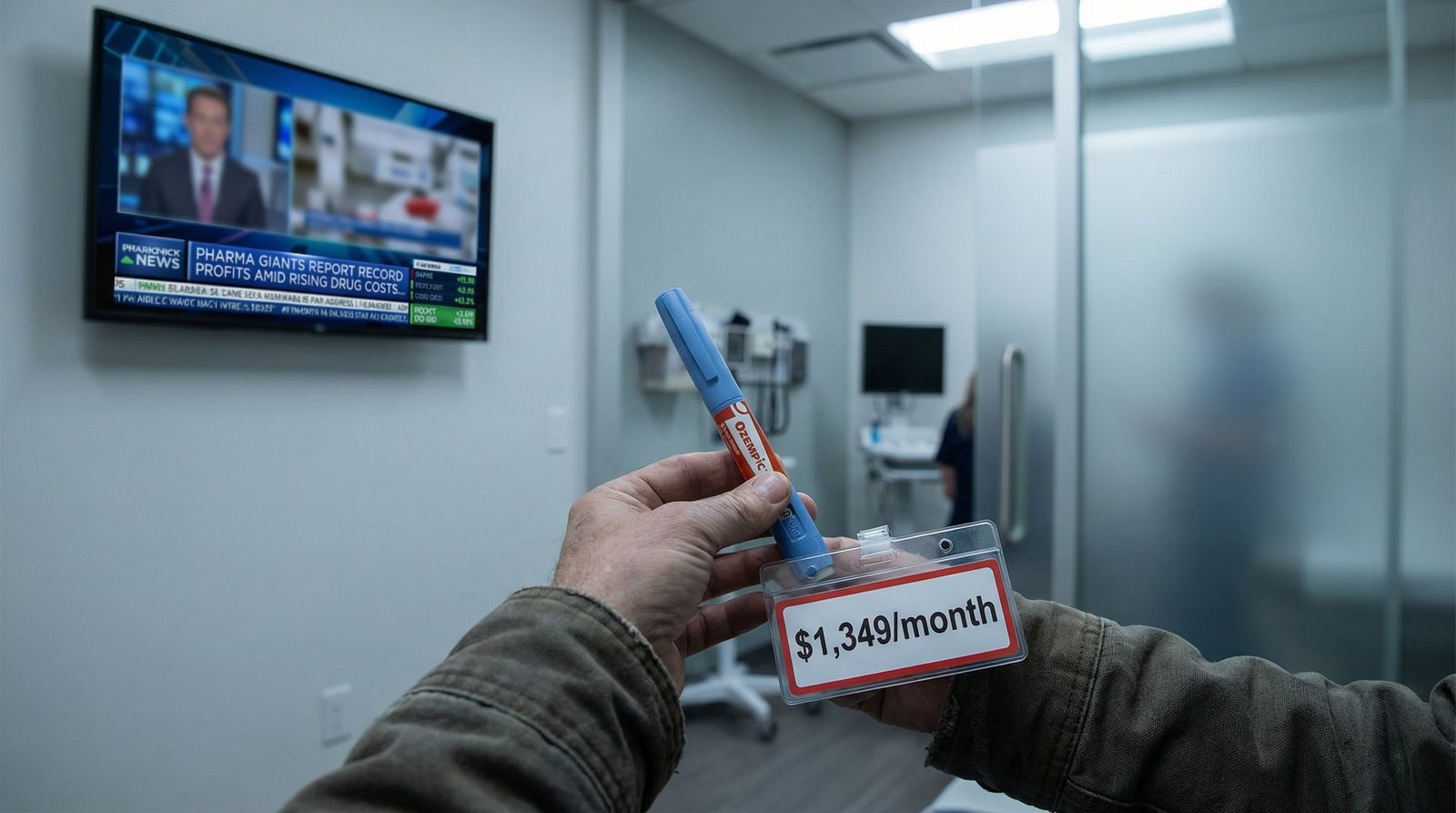
- Ozempic/Wegovy (semaglutide) costs $998–$1,349/month without insurance in America
- Drug companies raised list prices on new launches by 35% in 2023 alone
- Medicare negotiated its first 10 drug prices in 2026 — saving $6 billion annually, but Congress is already trying to roll it back
- Unlike every other wealthy nation, the US government is legally prohibited from negotiating drug prices across the board

The short answer: because Congress made it legal. Every other wealthy nation uses some form of government price negotiation or regulation to cap what pharmaceutical companies can charge. The United States, alone among developed nations, has largely prohibited its government from doing the same — and the drug industry spent decades lobbying to keep it that way.
Here’s the mechanism that makes American drug pricing uniquely predatory:
Per capita pharmaceutical spending in the US stands at $1,491 annually — compared to $995 in Germany, $962 in Switzerland, $893 in Canada, and $847 in Japan. Americans aren’t sicker. They’re not getting better drugs. They’re just paying more for the same products so that shareholders can collect larger dividends.
Insulin is the starkest example of how American prescription drug pricing isn’t about research costs — it’s about extraction. Insulin has existed since the 1920s. The scientists who developed it sold the patent for $1 because they wanted it to be universally available. Today, a single vial of insulin costs over $300 in the United States and under $35 in Canada — an 88% price difference for an identical product.
A RAND Corporation study found that US insulin prices average five to ten times higher than in other OECD countries. Over an 11-year study period, the average cost per unit of insulin in the United States increased by 10.3% while the same insulin in Canada increased by 0.01%. Not a typo.
For Americans with Type 1 diabetes who need insulin to survive — not manage a condition, but literally survive — monthly out-of-pocket costs without insurance run $200 to $600 for multiple vials. People have died rationing insulin. The “innovation premium” argument doesn’t apply to a 100-year-old drug.
Three companies — Eli Lilly, Novo Nordisk, and Sanofi — control roughly 90% of the global insulin market. They coordinate pricing in a way that would be called a cartel in any other industry. In America, it’s called the free market.

The romanticized version of the American healthcare story is that the uninsured suffer most. The reality is messier: insured Americans are rationing medication too — because deductibles, copays, and formulary exclusions mean that “having insurance” doesn’t mean your drug is affordable.
A 2025 survey found that 21% of U.S. adults didn’t fill a prescription in the last year due to cost. Another 23% used an over-the-counter alternative instead of a prescribed drug. These aren’t the unhoused or uninsured — they’re working people with jobs and health plans who discovered their plan doesn’t cover what their doctor ordered at a price they can afford.
The generational dimension is real but counterintuitive. Seniors on Medicare have been largely protected from the worst pricing through Part D plans and manufacturer discount programs — though the 25 most common Medicare drugs still increased 98% in price over 11 years. Working-age Americans on employer insurance face high deductibles, narrow formularies, and prior authorization delays. Young adults in the coverage gap — earning too much for Medicaid, too little for comfortable premiums — pay full list price or go without.
The people most exposed to unregulated prescription drug prices are Millennials and Gen Z adults in the gig economy, self-employed, or in jobs without benefits — exactly the people the gig economy dismantled benefits for. A generation told to bootstrap their way to prosperity is rationing blood pressure medication because the monthly cost eats into rent.

The pharmaceutical industry’s standard defense of high US prices is that American revenue subsidizes global research and development — that without charging Americans $300 for insulin, nobody would have funded insulin in the first place. This argument is worth examining against actual numbers.
Total US prescription drug spending hit $805.9 billion in 2024 — up 10.2% from 2023. That’s not R&D spending. That’s total retail and hospital drug expenditure. New drug launches in 2023 debuted at prices 35% higher than 2022 launches on average — not because of new research costs, but because the market allows it.
The five largest pharmaceutical companies collectively spent more on stock buybacks and dividends between 2016 and 2020 than on research and development. Johnson & Johnson, Pfizer, AbbVie, Merck, and Bristol-Myers Squibb repurchased $110 billion of their own stock in a five-year period — money that went to shareholders, not labs. The “innovation subsidy” framing is a public relations construct built on top of a wealth transfer.
Meanwhile, the federal government — funded by taxpayer money — contributes billions annually to basic drug research through the NIH. Drug companies routinely license publicly-funded discoveries, develop them into commercial products, and then charge Americans the highest prices in the world for drugs American taxpayers helped invent. This is not a bug in the system. It’s the business model.

For the first time in US history, Medicare negotiated drug prices directly — a power granted by the Inflation Reduction Act of 2022 that the pharmaceutical industry spent years and hundreds of millions of lobbying dollars trying to prevent.
The first round of negotiations covered 10 drugs that together consumed nearly 20% of all Medicare Part D spending ($46.4 billion) in 2022. The results were meaningful: negotiated prices represented at least 38% discounts from 2023 list prices, projected to save Medicare beneficiaries $1.5 billion annually in out-of-pocket costs and the Medicare program $6 billion per year overall.
Those 10 drugs — including Eliquis, Enbrel, Jardiance, Januvia, and Xarelto — now have Medicare-negotiated prices effective in 2026. A second round of 15 additional drugs is being negotiated, with Ozempic (semaglutide) scheduled for the 2027 round. The 2026 Medicare out-of-pocket cap is now $2,100 — a genuine protection for seniors on fixed incomes.
But here’s the catch: the 2025 budget reconciliation bill (H.R. 1) included provisions that restrict which drugs Medicare can negotiate, expected to increase Medicare spending by at least $5 billion. The same Congress that spent years blocking negotiation is now weakening the first negotiation program that actually worked. The same bill also cuts Medicaid by hundreds of billions.
And critically: Medicare negotiation only helps people on Medicare. The 150 million Americans under 65 on private insurance, employer plans, or no coverage at all get none of these negotiated rates. The drug is still $1,200 at the pharmacy counter if you’re 45 and uninsured.

GLP-1 drugs like Ozempic and Wegovy (both brand names for semaglutide) have become the most talked-about medications in America — and the most expensive. Without insurance, semaglutide costs $998 to $1,349 per month in the United States. The same drug costs roughly $59/month in Germany and under $100/month in the UK.
Novo Nordisk manufactures semaglutide in Denmark, where they’re headquartered, and sells it to their home country’s national health service at a negotiated price. They then sell the identical product in the US at 10 to 20 times the price — because they can, because American law doesn’t stop them, and because American patients are trapped.
The prescription drug prices problem is especially acute for GLP-1 drugs because these medications have proven effectiveness not just for weight loss but for cardiovascular disease, type 2 diabetes management, and potentially other conditions. These aren’t lifestyle drugs. They’re becoming frontline treatments — and they’re effectively inaccessible to working-age Americans without generous employer insurance coverage or the financial resources to pay out of pocket.
The Wegovy manufacturer’s own website advertises a $149/month self-pay program for certain doses — which implicitly acknowledges the $1,349 list price is not a real market price but a ceiling designed to extract maximum revenue from insurance companies before discounting for everyone else. This is how American drug pricing works: set the ceiling at the moon, discount from there, and let the uninsured pay whatever they can’t negotiate away.
The pharmaceutical industry’s core defense is that high US prices fund the research that produces the drugs the rest of the world free-rides on. Without American pricing, the argument goes, there would be no new drugs for anyone.
This argument is partially true and largely dishonest. It’s true that US revenues contribute substantially to pharmaceutical R&D budgets — the US market generates a disproportionate share of global drug company profits. It is not true that:
Trump’s Most Favored Nation executive order (May 2025) attempted to peg US drug prices to the lowest price paid by any comparable country — an approach that would directly address the pricing gap. The pharmaceutical industry responded with lawsuits. The policy has had limited implementation. The fundamental problem — that American law gives drug companies pricing power that no other government grants — remains intact.
Every other wealthy country has decided that allowing pharmaceutical companies to charge whatever they want for drugs people need to survive is not, in fact, an acceptable expression of free-market principles. The United States is the holdout. American patients are paying for that exceptionalism.
Why are prescription drug prices so high compared to other countries?
The US lacks government price controls that exist in every other wealthy nation. Drug companies set their own list prices with no regulatory cap, resulting in prescription drug prices 3–10 times higher than in Canada, Germany, or Japan for identical medications.
Can I buy cheaper prescription drugs from Canada legally?
Personal importation of prescription drugs from Canada for personal use is technically prohibited by federal law but has not been actively enforced by the FDA for small quantities. Several states have passed importation programs, though federal approval for wholesale importation has been slow. Some Americans travel to Canada or Mexico to purchase medications legally at local prices.
Does Medicare drug price negotiation lower costs for everyone?
No — only for Medicare beneficiaries (65+). The 2026 negotiated prices for 10 drugs reduce out-of-pocket costs for seniors enrolled in Part D plans. Working-age Americans on private insurance or uninsured pay the same unregulated prices as before.
Why does insulin cost so much in the US?
Three companies control 90% of the insulin market and face no government price regulation in the US. Insulin that costs $35/vial in Canada sells for over $300 in the US — a price difference explained entirely by the legal and regulatory structure of American drug pricing, not by manufacturing costs or research expenses.
Data and reporting in this article draw from: SingleCare — 2026 Prescription Drug Statistics; Drug Channels — CMS Data: Six Trends Reshaping US Drug Spending (2026); California Health Advocates — Medicare Negotiated Drug Prices Now in Effect; CMS — Medicare Drug Price Negotiation: Selected Drugs and Negotiated Prices; World Population Review — Cost of Insulin by Country 2026; University of Pittsburgh CP3 — Insulin Price Comparisons: Canada vs. United States; White House — TrumpRx.gov Fact Sheet (Feb 2026); Fay Nutrition — How Much Does Semaglutide Cost?; The Conversation — Why Is US Health Care Still the World’s Most Expensive?




